Eurosurveillance, Volume 13, Issue 28, 10 July 2008
 )1
)1- Institute of Medical Microbiology and Hygiene, Austrian Agency for Health and Food Safety (AGES), Vienna, Austria
- Department of Hygiene, Microbiology and Social Medicine, Medical University Innsbruck, Innsbruck, Austria
- Viral Enteric and Emerging Diseases Laboratory, Center for Disease Control, Taipei, Taiwan
- Department of Paediatrics, Regional Hospital Leoben-Eisenerz, Leoben, Austria
Date of submission: 04 July 2008
Hamaguchi et al. recently reported on the on the occurrence of enterovirus type 71 (EV71) subgenogroup C4 in Japan [1]. According to the authors, this strain may have emerged in mainland China and in Taiwan. EV71 subgenogroup C4 has recently gained public health interest following reports of an ongoing outbreak in China and Vietnam in 2008: In June 2008, more than 176,000 cases of hand, foot and mouth disease (HFMD) were reported in China alone, and at least 24 deaths have been attributed to EV71 [2,3]. In the largest and most severe EV71-associated HFMD outbreak in Taiwan in 1998, 405 children had severe neurological complications and/or pulmonary oedema; 78 children died [4].
The genus enterovirus comprises poliovirus, coxsackievirus, echovirus, and enteroviruses 68-71. Based on molecular classification, human enteroviruses (HEV) are divided into groups A-D. There are now in excess of 100 types of EV. EV71 has been allocated to the group HEV-A (together with coxsackievirus A16 and some other coxsackie A-viruses) [5]. Both EV71 and coxsackievirus A16 virus can cause HFMD and herpangina, but only EV71 frequently leads to severe diseases, such as aseptic meningitis or poliomyelitis-like paralysis; fatal cases due to pulmonary oedema have been reported in neonates [6].
By molecular typing EV71 can be divided into three genogroups (A,B,C), the latter two being further sub-divided into B1-5 and C1-5 [7,8]. Currently genogroups B and C are co-circulating worldwide. Genotype C1 is predominating in Europe, but it can also be found in Australia, Malaysia and Singapore [9,10]. In China, Taiwan and Japan, the other genotypes are dominant, obviously replacing each other in circulation every one or two years [9,10].
Laboratory investigation in Austria
In Austria, the Agency for Health and Food Safety (AGES) serves as the national reference centre for laboratory diagnosis of poliomyelitis [11]. Between 1999 and 2007, 1,388 stool specimens from patients with acute flaccid paralysis (AFP) or aseptic meningitis were voluntarily submitted by hospitals, none of them yielding polio virus.
The number of reported AFP-cases in patients under 15 years-old per year was 12 in 1999 (0.87/100,000/year), 13 in 2000 (0.95/100,000/year), nine in 2001 (0.66/100,000/year), eight in 2002 (0.62/100,000/year), two in 2003 (0.16/100,000/year), seven in 2004 (0.53/100,000/year), three in 2005 (0.23/100,000/year), and nine in 2006 (0.69/100,000/year) [11]. The WHO requirement of testing two stool specimens (gained within two weeks after onset of paralysis) for enterovirus in at least 80% of AFP-cases was fulfilled in 2002 (88%) and in 2003 (100%).
Stool specimens were processed according to recommendations from the World Health Organization (WHO) listed in the WHO’s 'Polio laboratory manual' [12]. In brief, samples were treated with chloroform and antibiotics to remove bacteria and fungi. Cell cultures were inoculated, incubated at 36°C and observed for cytopathic effect (CPE) daily. When complete CPE was obtained, the infected cells were harvested and stored at -20°C until serological typing by neutralisation tests using a kit provided by the National Institute of Public Health and the Environment (RIVM), Bilthoven, the Netherlands.
Of the 1,388 stool samples, 201 yielded non-polio enteroviruses. A total of 181 viruses were available for molecular typing as described by Nix et al. [13]. For EV71-positive isolates, extended length VP1 gene sequences were amplified as described by Oberste et al. [14].
Retrospective analysis of enterovirus samples
On the basis of a general cooperation agreement signed between AGES and the Center for Disease Control (CDC) in Taipei in fall 2007, AGES decided to screen retrospectively Austrian enterovirus isolates collected in its acute flaccid paralysis surveillance programme for EV71. Molecular typing was performed by an AGES employee in February 2008 during a three week stay at the Viral Enteric and Emerging Diseases Laboratory at the CDC in Taipei, Taiwan. Analysing enteroviruses cultured from 181 clinical samples collected between 1999 and 2007, we detected EV71 in specimens from 16 patients (8.8%): EV71 genotype C1 was found in 14 cases, and genotype C4 in two cases.
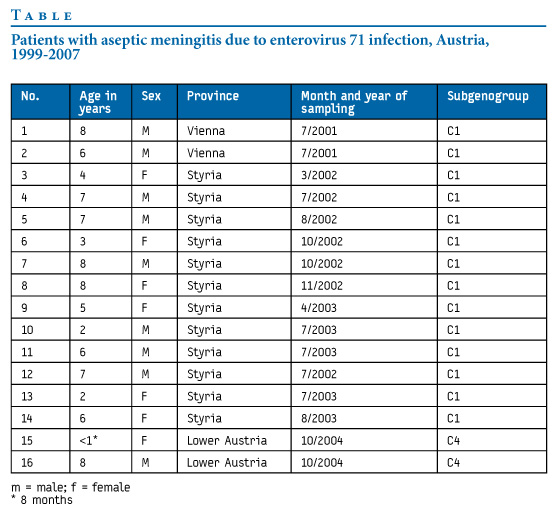
In the Austrian province of Lower Austria (1.5 million inhabitants), an eight year-old boy of Vietnamese descent (born and raised in Austria) and an eight month-old female breastfed infant, were hospitalised in October 2004 at different institutions for respective aseptic meningitis and aseptic meningitis plus diarrhoea. The two children lived in villages approximately 270 km apart, without any known common contacts; they were not known to have traveled abroad.
Table 1 summarises demographic data of the 16 patients with EV71 infection. No signs of HFMD were documented in any of them. All 16 Austrian patients with EV71 infection recovered completely.
Table. Patients with aseptic meningitis due to enterovirus 71 infection, Austria, 1999-2007
Discussion and conclusions
The discovery of two EV71 subgenogroup C4 isolates in Austria was an unexpected finding, as was the obvious occurrence of a cluster of infection with EV71 subgenogroup C1 in the years 2001-2003 in the province of Styria (1.2 million inhabitants). The fact that one of the two Austrian children suffering from EV71 subgenogroup C4 infection was of Vietnamese descent suggests that independent introduction of Asian strains may occur in Europe.
Several EV71 outbreaks have been documented throughout the world and clinical manifestations of EV71 infections can be diverse, including HFMD, herpangina, central nervous system (CNS) disease, and pulmonary oedema [1]. In children, the CNS diseases associated with EV71 manifest clinically in various ways, such as aseptic meningitis or acute flaccid paralysis, symptoms previously well known for infections with poliovirus. After the eradication of wild poliovirus from most parts of the world, EV 71 must be regarded as one of the most dangerous neurotropic enteroviruses. The well established WHO PolioLabNet may be well advised to upgrade for surveillance of EV71. Enterovirus surveillance is already an integral activity in some European polio laboratories.
References
- Hamaguchi T, Fujisawa H, Sakai K, Okino S, Kurosaki N, Nishimura Y, et al. Acute encephalitis caused by intrafamilial transmission of enterovirus 71 in adult. Emerg Infect Dis. 2008;14(5):828-30.
- Chinese Center for Disease Control and Prevention and the Office of the World Health Organization in China. Report on the Hand, Foot and Mouth Disease Outbreak in Fuyang City, Anhui Province and the Prevention and Control in China. May 2008. Available from: http://www.wpro.who.int/NR/rdonlyres/591D6A7B-FB15-4E94-A1E9-1D3381847D60/0/HFMDCCDC20080515ENG.pdf
- United States Centers for Disease Control and Prevention (CDC). Hand, foot and mouth disease – asia (19): CDC Notice. ProMED-mail. 4 July 2007. Archive no. 20080704.2037. Available from: http://www.promedmail.org/pls/otn/f?=2400:1202:2646754013195931::NO::F2400_P1202_CHECK_DISPLAY,F2400_ P1202_PUB_MAIL_ID:X,73018
- Ho M, Chen ER, Hsu KH, Twu SJ, Chen KT, Tsai SF, et al. An epidemic of enterovirus 71 infection in Taiwan. Taiwan Enterovirus Epidemic Working Group. N Engl J Med. 1999;341(13):929-35..
- Wu TC, Wang YF, Lee YP, Wang JR, Liu CC, Wang SM, et al. Immunity to avirulent enterovirus 71 and coxsackie A16 virus protects against enterovirus 71 infection in mice. J Virol. 2007;81(19):10310-5.
- Ho M. Enterovirus 71: the virus, its infections, and outbreaks. J Microbiol Immunol Infect. 2000;33(4):205-16.
- Mizuta K, Abiko C, Murata T, Matsuzaki Y, Itagaki T, Sanjoh K, et al. Frequent importation of enterovirus 71 from surrounding countries into the local community of Yamagata, Japan, between 1998 and 2003. J Clin Microbiol. 2005;43(12):6171-5.
- Tu PV, Thao NT, Perera D, Huu TK, Tien NT, Thuong TC, et al. Epidemiologic and virologic investigation of hand, foot, and mouth disease, southern Vietnam, 2005. Emerg Infect Dis. 2007;13(11):1733-41.
- Cardosa MJ, Perera D, Brown BA, Cheon D, Chan HM, Chan KP, et al. Molecular epidemiology of human enterovirus 71 strains and recent outbreaks in the Asia-Pacific region: comparative analysis of the VP1 and VP4 genes. Emerg Infect Dis. 2003;9(4):461-8.
- Sanders SA, Herrero LJ, McPhie K, Chow SS, Craig ME, Dwyer DE, et al. Molecular epidemiology of enterovirus 71 over two decades in an Australian urban community. Arch Virol. 2006;151(5):1003-13.
- Strauss R, Sagl M, Wewalka G, Dierich M, Baumhackl U, Holzmann H, et al. WHO Polio Eradication Programme: Status quo and implementation in Austria. [In German]. Wien Klin Wochenschr. 2008;120(7-8):210-6.
- World Health Organization. Polio laboratory manual. 4th edition. Geneva; 2004. Available from: http://www.who.int/vaccines/en/poliolab/WHO-Polio-Manual-9.pdf
- Nix WA, Oberste MS, Pallach MA. Sensitive, seminested PCR amplification of VP1 sequences for direct identification of all enterovirus serotypes from original clinical specimens. J Clin Microbiol. 2006;44(8):2698-704.
- Oberste MS, Maher K, Kilpatrick DR, Pallansch MA. Molecular evolution of the human enterovirus: correlation of serotype with VP1 sequence and application to picornavirus classification. J Virol. 1999;73(3):1941-8






